




The 60-kDa Shadow Over Your Blood Pressure: Why Direct Angiotensinogen (AGT) Quantification — Not Just Renin or ANG II — Is the REAL RAS Baseline Your Experiment Is Missing
If the Renin–Angiotensin–Aldosterone System (RAAS/RAS) is the most pharmacologically exploited signaling network in human medicine, then angiotensinogen (AGT) is the quiet flood it all floats on — and the one variable most labs still measure indirectly when they should be measuring it directly. Every second of every day, ~25–40 µg/mL (mg/L range) of this 452-aa, ~60 kDa α₂-globulin circulates in human plasma, constitutively secreted by hepatocytes, waiting for a single, fateful cleavage: renin peels off the N-terminal decapeptide ANG I, ACE then converts ANG I → ANG II, and the vasopressor cascade that controls vascular tone, sodium balance, and organ perfusion is off to the races. Yet ironically, for a molecule so central, most hypertension, nephrology, and cardiovascular research still chases PRA (plasma renin activity via ANG I generation), plasma renin concentration (PRC via immunoassay), or ANG II mass spectrometry, while treating AGT — the substrate — as a constant. It isn't. AGT rises with glucocorticoids, estrogens, thyroid hormone, and inflammatory cytokines; it shifts with plasma volume expansion/contraction; and its plasma level is independently associated with essential hypertension severity, preeclampsia risk, and renal tubular development disorders. The Human Angiotensinogen (AGT) ELISA Kit (KTE60968) from Abbkine is the tool that finally puts AGT on your plate as a calibrated, sandwich-ELISA variable — no more inferring the substrate from the enzyme or assuming it's "flat."
AGT: The Non-Inhibitory Serpin That Runs the Show
Angiotensinogen (UniProt: P01019, Gene ID 183, alias SERPINA8 / ANHU) looks like a serpin (serine protease inhibitor) on paper — it carries the conserved serpin fold, the reactive-center loop region, and migrates as an α₁-globulin on protein electrophoresis — but it is not an enzyme inhibitor in the classical sense. Its "reactive center" is actually the Leu⁻Val bond at positions 10–11 of the mature angiotensin sequence — the scissile site that renin (a highly specific aspartic protease, NOT a serine protease) recognizes to release ANG I. This is a beautiful paradox: AGT sits in the serpin superfamily phylogenetically, but its sole job is to serve as the obligatory substrate reservoir for the one protease that controls blood pressure at the first step.
Key biological facts that explain why plasma AGT levels matter:
• >90% of circulating AGT is made in the liver (hepatocytes), with tiny contributions from adipose, kidney, brain, and vascular tissue locally.
• Plasma AGT is ~25–40 mg/L in healthy humans, meaning its concentration far exceeds renin's catalytic capacity — substrate is rarely rate-limiting in the short term, but chronically altered AGT (genetically or hormonally) shifts steady-state ANG I/II production and resets the entire RAS gain knob.
• Estrogen increases AGT transcription (one reason plasma ANG levels shift in pregnancy and why oral contraceptives can nudge BP).
• Mutations in AGT are linked to susceptibility to essential hypertension; severe loss-of-function disrupts renal tubular development (renal tubular dysgenesis).
Why You Need a Sandwich ELISA for AGT (And Why Indirect RAS Readouts Fall Short)
Renin activity assays (PRA) and ANG II LC-MS/MS are powerful — but they come with blind spots:
What You Measure What It Misses
PRA (ANG I generation rate) Assumes AGT is constant & saturating; doesn't quantify substrate directly
Plasma renin concentration (PRC) Proximity-based, ignores whether substrate availability shifted
ANG II mass (MS/ELISA) Downstream readout; can't tell if ANG levels are high because renin is high or because AGT substrate is high
Direct AGT ELISA Gives you the [Substrate] term itself — lets you compute effective RAS substrate capacity, normalize PRA to AGT, and catch hormonal/volumetric shifts that alter AGT independently
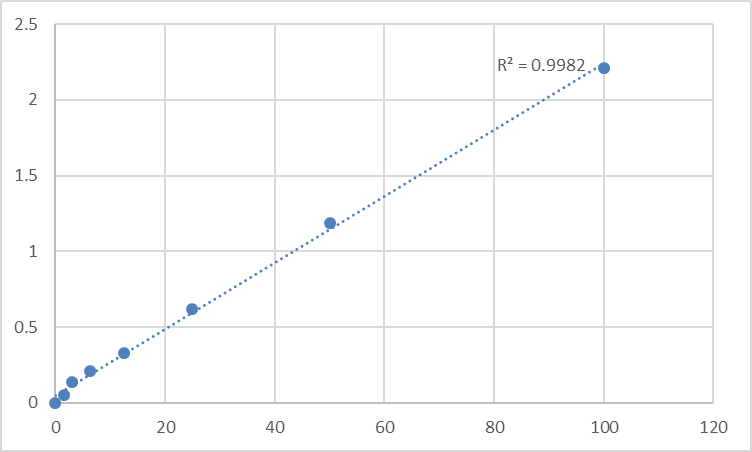
The KTE60968 kit uses the field-standard two-site sandwich ELISA:
- Microplate pre-coated with a capture antibody specific for human AGT.
- Standards + samples (serum, plasma, other biological fluids) → AGT binds.
- Wash → add biotinylated anti-AGT detection antibody (different epitope).
- Streptavidin–HRP → TMB → color ∝ [AGT].
- Stop → read 450 nm → interpolate from the recombinant AGT standard curve.
From distributor/technical sheets that match this product line, the operating specs cluster around:
Parameter Typical Specification
Target Human Angiotensinogen / AGT (P01019, SERPINA8)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → SA-HRP → TMB, 450 nm
Dynamic Range 1.56 – 100 ng/mL (kit standard curve; plasma is well above this, so samples are diluted into range — typical 1:200–1:500 pre-dilution of serum/plasma)
Sensitivity / LOD ~0.6–0.94 ng/mL
Intra-Assay CV ≤ ~5.4%
Inter-Assay CV ≤ ~8.3%
Specificity No significant cross-reactivity with analogues
Samples Serum, plasma (EDTA preferred), tissue homogenates, cell culture supernatants, other biological fluids
Assay time ~3–5 hours
Where Direct AGT Measurement Actually Moves the Needle
- Essential & secondary hypertension research
AGT plasma levels rise with insulin resistance, visceral adiposity, and steroid excess — but not always proportionally to renin, which is why PRA/AGT ratios and simply knowing the substrate mass refines your RAS phenotyping. It also matters for RAAS blockade pharmacology: ACEi/ARB shift ANG feedback → renin ↑, but AGT response can lag or adapt — best tracked with a calibrated ELISA, not assumptions.
- Preeclampsia & pregnancy-associated hypertension
Pregnancy is the ultimate endocrine/volumetric confounder: estrogen drives hepatic AGT ↑, plasma volume expands, and yet preeclampsia shows dysregulated RAS/vascular reactivity. Having serial AGT + PRA/ANG I + sFlt-1/PlGF on the same cohort lets you separate "normal pregnancy RAS remodeling" from "pathogenic endothelial dysfunction."
- Liver-centric RAS modulation & hepatokine biology
Because AGT is a hepatokine (liver secretory product), conditions affecting hepatocyte function — NASH, cirrhosis, portal hypertension, IL-6 inflammatory states — can shift circulating AGT independent of renin. Quantifying it connects systemic RAS to hepatic inflammation (IL-6 → STAT3 → AGT transcription via the acute-phase response).
- Sepsis, shock & plasma volume studies
Massive fluid shifts dilute or concentrate AGT artifactually if you read it as a "hormone concentration" without correcting for hemoconcentration/dilution. But that's exactly why you want the direct number: paired with total protein/albumin or dilution markers, it becomes the tool to disentangle true synthesis changes from volume artifact.
- Genetic & CRISPR vascular models
If you're working on AGT promoter variants, miR-122/miR-155 regulation of hepatocyte AGT, or liver-specific AGT knockout (floxed AGT mouse → albumin-Cre), the readout is simple: how much AGT is left in circulation or in conditioned hepatoctye media? An ELISA gives you ng/mL ± SEM across genotypes/doses — far more persuasive than a semi-quantitative band.
A Quick Sample-Prep Note (Because Plasma AGT Is ~mg/L, Not ng/L)
Unlike a cytokine at pg/mL, AGT sits so high in plasma that the key operational rule is: dilute correctly.
• EDTA plasma preferred for RAS work (EDTA chelates Ca²⁺, minimizes ex vivo ANG II generation and protease crosstalk).
• Pre-dilute serum/plasma into the kit's Assay Buffer (commonly 1:200–1:500 to land inside the 1.56–100 ng/mL standard curve) — always verify the exact dilution factor on your lot's manual.
• Include a pooled normal plasma as internal control on every plate so inter-plate drift is trackable.
• Warm reagents to RT ≥ 30 min, read 450 nm promptly after stop, and fit a 4-PL or linear regression for the standard curve.
The Bottom Line
AGT is the 60-kDa substrate reservoir that makes the entire renin–angiotensin system possible — the most abundant RAS protein in human blood, liver-derived, estrogen- and cytokine-responsive, and functionally inseparable from how we understand hypertension, preeclampsia, liver inflammation, and volume homeostasis. Measuring it directly, with a two-site sandwich ELISA that gives you a plate-readable ng/mL, transforms it from a theoretical constant into a real experimental variable. The Human Angiotensinogen (AGT) ELISA Kit — KTE60968 from Abbkine is built for exactly that job: pre-coated capture → biotin detection → HRP–TMB → 450 nm → AGT concentration, in a 3–5 hour workflow that scales from a clinical-pilot cohort to a mechanism-of-action study.
Product Reference: KTE60968 – Human Angiotensinogen (AGT) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-angiotensinogen-agt-elisa-kit-kte60968/
(For Research Use Only; not for diagnostic procedures in humans.)





