




The ER's Calcium-Tuned Secretory Chaperone You're Probably Ignoring: Why RCN2/ERC-55 Quantification Changes How You Read Fibrosis, Cancer Secretion, and ER Stress
Every time a secretory or membrane protein folds inside the endoplasmic reticulum, it's doing so in a calcium-rich luminal bath that must be actively buffered, sensed, and tuned — and the protein most quietly holding that environment together is RCN2, better known as Reticulocalbin-2, ERC-55 (Endoplasmic Reticulum Calcium-binding protein of 55 kDa), or E6BP (E6-binding protein). Despite the alphabet soup of aliases, RCN2 has a very clear anatomical address: it's a luminal ER protein (C-terminal HDEL retention signal) carrying six EF-hand Ca²⁺-binding motifs, and it belongs to the CREC family (Cab45 / reticulocalbin / calumenin) that acts as the ER's low-affinity calcium sensor and secretory-quality control scaffold. What makes it suddenly relevant to modern PI labs isn't just "calcium binding" — it's that RCN2 protein levels are now directly tied to TGF-β–driven fibrogenesis, EMT and tumor progression, and even HPV oncoprotein hijacking (via the E6BP interaction). But because it's an ER-luminal residents you can't see from outside without the right tool, most labs stop at mRNA or a semi-quantitative Western. The Human Reticulocalbin-2 (RCN2) ELISA Kit (KTE60815) from Abbkine closes that gap: a two-site sandwich ELISA that turns this elusive EF-hand scaffold into a calibrated ng/mL readout you can normalize, replicate, and — critically — correlate with your functional ER stress, secretion, and TGF-β phenotypic data.
RCN2 / ERC-55 / E6BP: What It Actually Is (And Why It Has Three Names)
RCN2 (UniProt: P34956, Gene ID: 5955, 15q24.3) is synthesized with an N-terminal signal sequence that directs it into the ER lumen, and it never leaves because its C-terminal HDEL tetrapeptide continuously retrieves it through the KDEL receptor cycling system. Inside the lumen, its six EF-hand motifs (some functional, some structural) allow it to bind Ca²⁺ and participate in the calcium-dependent folding environment that calreticulin, calnexin, and ERp57 also depend on.
The three most-used names each tell a different story:
• ERC-55 = the historical biochemical name (Endoplasmic Reticulum Calcium-binding protein of 55 kDa — apparent mass on SDS-PAGE)
• Reticulocalbin-2 / RCN2 = the genomics-family name (related to the original reticulocalbin/RCN1 but distinct)
• E6BP = the virology-functional name: it was cloned as the cellular binding partner of HPV E6 oncoprotein, explaining how high-risk HPV subverts ER-resident checkpoints during cervical transformation
Functionally, RCN2 is implicated in calcium homeostasis, secretory protein folding/quality control, redox-modulated ER signaling, and regulation of TGF-β responses — the last of which is why it keeps appearing in hepatic stellate cell activation, liver fibrosis, and colorectal EMT datasets.
Why You Need a Sandwich ELISA for RCN2 (And Why a Western Alone Won't Cut It)
RCN2 is not a secreted cytokine you scoop from media — it's ER-luminal, so to measure it you're almost always working with cell/tissue lysates or membrane/organelle-enriched fractions, and its abundance is moderate but not "housekeeping protein" abundant. That creates three practical problems for gel-only approaches:
- Loading normalization fights: if your ER expands/contracts under stress (tunicamycin, thapsigargin, TGF-β, hypoxia), total protein per cell shifts, and "Actin-normalized band density" can mislead.
- Multiple EF-hand paralogs in the CREC family mean single-antibody bands can be ambiguous without a second orthogonal epitope.
- Replicates & cohorts: you can't realistically Western 40+ samples with good quantitative confidence; a 96-well sandwich ELISA lets you run time courses, dose responses, and patient-cohort tissue lysates in one sitting.
KTE60815 solves these by using a pre-coated capture antibody + biotinylated detection antibody (different epitope) → Streptavidin–HRP → TMB, 450 nm → interpolate from a recombinant RCN2 standard curve.
Assay Principle: The KTE60815 Sandwich ELISA
- A microplate is pre-coated with an anti-RCN2 capture antibody.
- Standards + samples (serum, plasma, tissue homogenates, cell lysates, culture supernatants, other biological fluids) are added; RCN2 present binds.
- After wash → biotinylated anti-RCN2 detection antibody forms the sandwich.
- Streptavidin–HRP → TMB → color ∝ bound RCN2.
- Stop solution → read 450 nm → interpolate ng/mL from the standard curve.
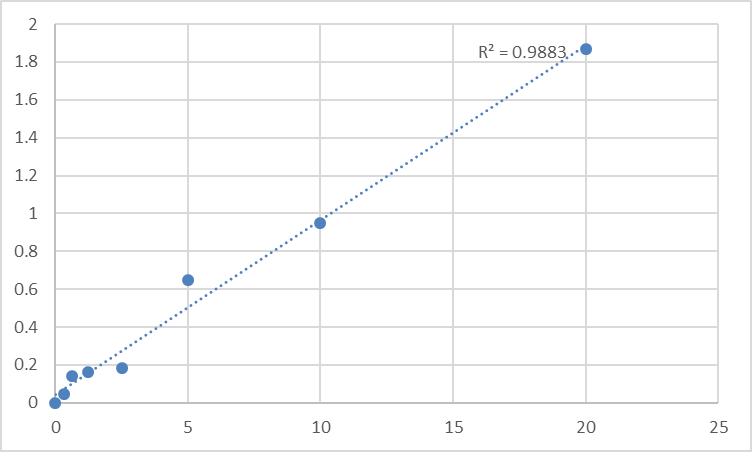
Representative performance envelope reported for this kit family:
Parameter Typical Value
Detection Range 0.312 – 20 ng/mL
LOD / Sensitivity ≤ ~0.112–0.16 ng/mL
Intra-Assay CV < 10%
Inter-Assay CV < 12–15%
Specificity No significant cross-reactivity with analogues
Samples Serum, plasma, tissue homogenates, cell lysates, culture supernatants, other biological fluids
Assay time ~3–5 hours
(Always anchor your Methods to the lot-specific certificate that ships with your kit.)
Where Quantifying RCN2 Protein Actually Moves the Needle
- Liver fibrosis & stellate cell activation
Multiple lines of evidence tie RCN2/ERC-55 upregulation to TGF-β–stimulated fibrogenic programs — it appears in activated hepatic stellate cells and fibrotic tissue contexts, where ER Ca²⁺ handling and secretory folding load track with collagen I/α-SMA outputs. ELISA lets you put a ng/mg total protein number on that, not just a microarray hit.
- Colorectal cancer & EMT-driven metastasis
RCN2 overexpression has been reported as correlated with tumor metastasis and poorer prognosis in CRC cohorts, with mechanistic links to EMT promotion — again, the protein-level readout is what validates whether the ER chaperone/scaffold is actually accumulating in the tissue you're sectioning.
- HPV oncoprotein / E6BP biology
Because RCN2 is literally E6BP (the E6-binding partner), any lab working on HPV16/18 E6-mediated transformation, p53-independent routes, or ER-resident checkpoint bypass benefits from quantifying the bait protein itself in transfected vs. primary keratinocyte lysates.
- ER stress & secretion-quality-control screens
If you're screening ER stressors (tunicamycin, Brefeldin A, disulfide disruptors) or CRISPR hits in CREC-family genes, RCN2 is a natural "second-order" marker of how the ER lumen's Ca²⁺-sensor layer responds — best read as a calibrated concentration, not a fold-change eyeball.
- Normalization sanity
Express RCN2 as ng RCN2 / mg total protein (BCA) or, if you're isolating ER-enriched fractions, as ng / μg ER-marker (e.g., calnexin/calreticulin) — either way, the ELISA gives you the denominator discipline a blot can't guarantee.
A Quick Prep Note That Protects Your Data
Since RCN2 is ER-luminal and often discussed in the context of microsomal/membrane fractions:
• Lyse cold in a protease-inhibitor-supplemented buffer; if you want the "true ER pool," a post-nuclear supernatant → high-speed spin (100,000×g pellet = microsomes) is ideal, but even a well-clarified whole-cell lysate works for most comparative studies.
• BCA the same lysate → report ng RCN2 / mg total protein.
• Aliot, avoid >2 freeze–thaw cycles, and warm all kit reagents to RT ≥ 30 min before opening.
• Run the full standard curve on every plate — never reuse a curve from a different day.
The Bottom Line
RCN2/ERC-55/E6BP is one of those proteins that sits at the intersection of ER calcium sensing, secretory folding, fibrotic activation, and viral oncoprotein hijack — but its ER-luminal address means it stays invisible unless you measure it properly. The Human Reticulocalbin-2 (RCN2) ELISA Kit (KTE60815) from Abbkine gives you that visibility: pre-coated capture → biotin detection → HRP–TMB → 450 nm → ng/mL, in a ~3–5 h workflow that scales from a tunicamycin time-course to a 50-sample tissue cohort without chaining you to a gel rig.
Product Reference: KTE60815 – Human Reticulocalbin-2 (RCN2) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-reticulocalbin-2-rcn2-elisa-kit-kte60815/
(For Research Use Only; not for diagnostic procedures in humans.)





