




More Than Just "Salt and Water": Why ENaC-γ (SCNN1G) Protein Quantification Is the Missing Variable in Hypertension, Kidney, and Airway Research
If you ask most people what the epithelial sodium channel does, they'll say "kidney — it reabsorbs sodium, duh." And sure, that's true — but it's also like saying the Ferrari engine is "mostly for making loud noises." The amiloride-sensitive epithelial Na⁺ channel (ENaC) is one of the most selective, tightly regulated ion gates in human biology, and its γ subunit (SCNN1G / γ-ENaC / ENaCγ, UniProt: P51170, ~649 aa, mature ~74–80 kDa with N-glycosylation) is the structural linchpin that decides whether this channel gets trafficked, stabilized, and retrieved at exactly the right apical surface — or runs constitutively open and floods the body with hidden sodium. When SCNN1G goes wrong genetically (truncation or PY-motif abolition → failed NEDD4-2/NEDD4L ubiquitylation → ENaC escapes endocytosis), you get Liddle syndrome (MIM:177200 / LIDLS2): early-onset hypertension, hypokalemic metabolic alkalosis, suppressed renin/aldosterone, and a kidney that simply refuses to stop pulling Na⁺ back from the urine. But even outside rare monogenic disease, ENaC-γ protein levels are the proximal readout of sodium-homeostasis control across the distal nephron, the airway epithelium, the colonic mucosa, and the sweat gland — which is why having a calibrated sandwich ELISA for it changes the conversation from "we assume ENaC is active" to "we measured the subunit that gates it."
ENaC: The Tri-Subunit Gatekeeper of Epithelial Na⁺ Reabsorption
ENaC is a heterotrimer (αβγ) — sometimes δβγ in specific non-classical contexts — held together at the apical plasma membrane of high-resistance epithelia. Each subunit is a multi-pass (8 TM) membrane protein with cytoplasmic N- and C-termini; the pore itself is formed primarily by the α subunit, but β and γ are essential for proper folding, forward trafficking, proteolytic activation, and regulated retrieval via their intracellular PY motifs (PPxY) that recruit WW-domain E3 ligases like NEDD4/NEDD4L.
Why γ (SCNN1G) specifically matters:
• It carries a critical conserved PY motif whose disruption is the molecular signature of many Liddle syndrome–causing mutations (C-terminal truncations or missense changes that break PPxY → ENaC can't be ubiquitylated → it piles up at the membrane → Na⁺ retention → volume expansion → HTN).
• Its extracellular loops are sites of proteolytic "activation cleavage" (e.g., by furin, prostasin/PRSS8, cathepsin D) that lock ENaC into a high-Po state — a process dysregulated in cystic fibrosis airway disease (hyperactive ENaC → ASL dehydration → mucus stasis → infection).
• Its palmitoylation and lipid interactions (notably with PIP₂ via β/γ subunits) modulate channel open probability — meaning total γ-ENaC protein at the apical membrane is often the best proxy for "how much functional channel is actually sitting where it counts".
Why a Sandwich ELISA for SCNN1G — And Why It's Tougher (and More Valuable) Than a Secreted Protein
Unlike a cytokine that floats free in media, SCNN1G is a multi-pass membrane protein — it lives buried in the apical membrane, often in relatively low copy, and its "concentration" in a tissue lysate is really a membrane-density question. That means:
- You need two epitopes (capture + detection) because a single antibody can get confused by homologous regions in α/β subunits or by partially degraded fragments running at ~50–60 kDa.
- Sample prep is half the battle — crude whole-cell lysates dilute the signal below detection, whereas membrane-enriched fractions, BBMV (brush-border membrane vesicles), or well-clarified apical-enriched lysates put the subunit where the ELISA can see it.
- Total-protein normalization (BCA) is non-negotiable — you'll want pg or ng ENaC-γ per mg total protein, not just "lysate ng/mL," to make inter-sample comparisons defensible.
The payoff? You can now run kidney cortex vs. medulla, aldosterone-treated vs. control, sgRNA-rescue vs. truncation-mutant, drug-treated airway epithelia (Calu-3/primary bronchial epithelia) on a 96-well plate and get a real number — not a "dark band vs. light band" argument.
Assay Principle: The KTE60735 Sandwich ELISA
The Human Amiloride-sensitive Sodium Channel Subunit Gamma (SCNN1G) ELISA Kit (KTE60735) uses the classic two-site architecture:
- A microplate is pre-coated with a capture antibody specific for human SCNN1G.
- Standards and samples (serum, plasma, tissue homogenates, cell lysates, cell culture supernatants/lysates, other biological fluids) are added; SCNN1G present binds.
- After washing, a biotinylated anti-SCNN1G detection antibody (different epitope) forms the sandwich.
- Streptavidin–HRP → TMB → color ∝ bound SCNN1G.
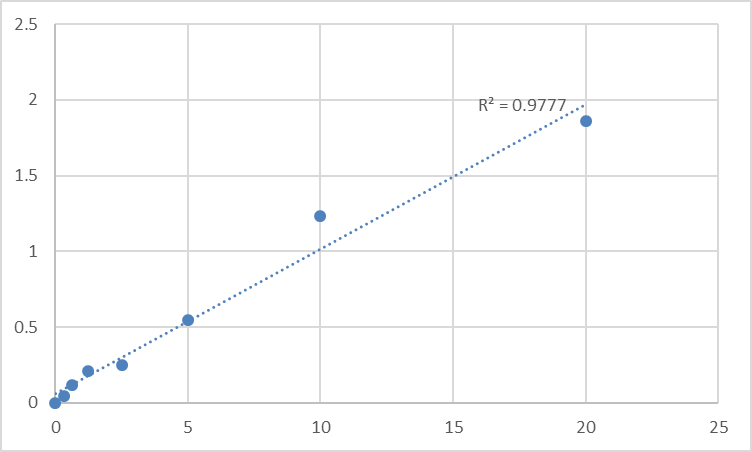
- Stop solution → read Absorbance at 450 nm → interpolate unknowns from the recombinant SCNN1G standard curve.
Reported operating envelope from distributor/technical summaries that mirror this kit's design space:
• Detection Range: 0.312 – 20 ng/mL
• Sensitivity / LOD: ≤ ~0.112–0.16 ng/mL
• Intra-/Inter-Assay CV: low-double-digit %, with no significant cross-reactivity to other ENaC subunits reported
• Assay Duration: ~3–5 hours (standard sandwich ELISA workflow)
• Samples: serum, plasma, tissue homogenates, cell culture supernates/lysates, other biological fluids
• Status: For Research Use Only — NOT for human clinical diagnosis
Where Quantifying ENaC-γ Protein Actually Moves Your Paper Forward
- Salt-sensitive hypertension & Liddle syndrome modeling
Quantify SCNN1G protein in kidney-cortex or distal-nephron-enriched lysates/BBMVs from mouse models, patient-derived slices, or CRISPR-edited kidney cells to correlate allelic variants / PY-motif mutations with channel surface density. ELISA gives you the numerical bridge between "DNA change" and "channel that won't leave the membrane."
- Nephrology transport physiology (aldosterone, K⁺, acid-base)
ENaC is aldosterone-regulated (via SGK1/NEDD4-2 relief-of-inhibition). Tracking γ-ENaC levels across NaCl restriction, K⁺ loading, acidosis/alkalosis, or MR-antagonist (spironolactone/eplerenone) treatment turns a black-box transporter into a measured variable.
- Airway surface liquid (ASL) & CF research
In cystic fibrosis and related mucociliary disorders, hyperactive ENaC is a drug target (amiloride itself is used clinically; P2Y2-receptor agonists like denufosol were evaluated to stimulate Cl⁻/fluid secretion). Being able to quantify SCNN1G in airway epithelial lysates or apical-bathing fluid fractions adds a protein-level readout to Ussing-chamber I_SC measurements.
- Colon, sweat gland & salivary epithelium studies
These "non-kidney" ENaC sites matter for CFTR–ENaC cross-talk, CF comorbidities, and even taste perception (ENaC in taste buds). If your model works on colonic Na⁺ absorption, diarrhea/secretory states, or CF-related sweat-test biology, γ-ENaC protein is part of that story.
- sgRNA / AAV gene-therapy validation
Editing SCNN1G (or rescuing Liddle-type truncations with mini-genes)? Report % γ-ENaC protein remaining (or rescued) ± SEM from a calibrated curve — reviewers notice the difference between "band looks back" and "4.8 ng/mg total protein restored, p < 0.01."
A Quick Prep Blueprint So Your OD₄₅₀ Reflects Biology, Not Debris
• BBMV / membrane enrichment pays off: homogenize in hypotonic buffer + protease inhibitors, Mg²⁺/Percoll gradients or differential spins → keep the apical-membrane fraction cold and clarified.
• Run BCA on the same final lysate; express SCNN1G as ng per mg total protein (or pmol/mg if you push sensitivity).
• Warm all kit reagents to RT ≥ 30 min before opening; protect TMB from light; stop uniformly; read 450 nm promptly.
• Always run the full standard curve on every plate — membrane-preparation variance is exactly why you don't reuse Tuesday's curve.
The Bottom Line
ENaC is the reason your kidney can reabsorb sodium without frying your blood pressure — and SCNN1G (γ-ENaC) is the subunit that decides whether that gate stays gated or runs wide open. Whether you're studying Liddle syndrome genetics, aldosterone signaling, CF airway dehydration, or epithelial transport in any high-resistance tissue, measuring γ-ENaC as a calibrated, plate-readable concentration instead of a guess on a gel is the upgrade that makes the story hold up. The Human Amiloride-sensitive Sodium Channel Subunit Gamma (SCNN1G) ELISA Kit — KTE60735 from Abbkine gives you that upgrade: pre-coated capture → biotin detection → HRP–TMB → 450 nm → ng/mL, in a ~3–5 hour workflow that fits inside a real lab day.
Product Reference: KTE60735 – Human Amiloride-sensitive sodium channel subunit gamma (SCNN1G) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-amiloride-sensitive-sodium-channel-subunit-gamma-scnn1g-elisa-kit-kte60735/
(For Research Use Only; not for diagnostic procedures in humans.)





