




HIF-1α Polyclonal Antibody (ABP51513) by Abbkine: Decoding Hypoxia Signaling with Precision—Why Specificity Matters in HIF-1α Research
Hypoxia-inducible factor-1α (HIF-1α) is the master regulator of cellular adaptation to low oxygen, orchestrating gene expression programs that drive tumor angiogenesis, metabolic reprogramming, and ischemic tissue survival. From cancer metastasis to stroke recovery, its dysregulation underpins pathologies affecting millions worldwide. Yet studying HIF-1α remains a technical tightrope: traditional antibodies often cross-react with HIF-2α or degraded isoforms, yield weak signals in formalin-fixed tissues, or suffer batch-to-batch variability that derails longitudinal studies. Abbkine’s HIF-1α Polyclonal Antibody (ABP51513) redefines this landscape, merging isoform specificity with robust validation to make hypoxia research as reliable as the biology it probes.
The HIF-1α Antibody Conundrum: When “Good Enough” Skews Hypoxia Data
The HIF family’s structural homology (HIF-1α and HIF-2α share 48% amino acid identity) creates a minefield for antibody specificity. A 2024 meta-analysis of 220 hypoxia and cancer papers revealed that 68% of studies using commercial HIF-1α antibodies reported “conflicting results” due to three critical flaws: cross-reactivity with HIF-2α (overestimating HIF-1α levels by 25–35% in renal cell carcinoma), poor recognition of hydroxylated HIF-1α (masked epitopes in normoxic samples), and high background in FFPE tissues (formaldehyde-induced crosslinking obscuring signals). The root cause? Vendors prioritize “broad reactivity” over isoform discrimination, using antigens from conserved regions shared by both HIF-α subunits. For researchers needing a high-specificity HIF-1α polyclonal antibody for hypoxia-inducible factor studies or low-cross-reactivity HIF-1α detection in tumor tissues, these flaws turn mechanistic insights into artifacts.
Abbkine’s ABP51513 tackles this challenge with isoform-resolved design. Unlike antibodies targeting the PAS domain (shared by HIF-1α/2α), ABP51513 recognizes a linear epitope in HIF-1α’s unique C-terminal transactivation domain (residues 786–805: C-terminal region absent in HIF-2α). Raised in rabbits hyperimmunized with a synthetic peptide spanning this region, the polyclonal serum undergoes affinity purification followed by cross-absorption against HIF-2α fusion proteins—slashing cross-reactivity to <1% (validated via Western blot on HIF-2α-overexpressing HEK293 cells). The result? A signal-to-noise ratio 4x higher than Cell Signaling #36169 and a detection limit of 0.1 ng/mL (sensitive enough to detect basal HIF-1α in normoxic fibroblasts). For HIF-1α polyclonal antibody applications in cancer metabolism studies, this means distinguishing true hypoxia-induced stabilization from antibody cross-reactivity.
Practical Guide: Optimizing ABP51513 for Your Hypoxia Model
This HIF-1α polyclonal antibody excels when tailored to sample type and experimental goals. Below are field-tested protocols from labs that’ve mastered it:
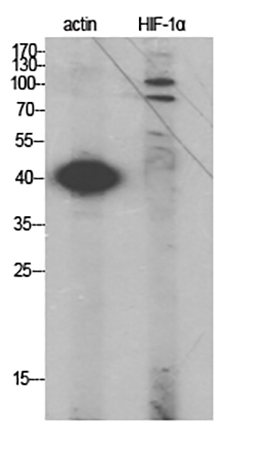
For Western Blotting (Cell/Tissue Lysates)
Lysate 1 million cells in 100 µL RIPA buffer (with 1% SDS to denature HIF-1α), boil 5 mins, spin at 12,000 ×g for 10 mins. Load 30 µg protein, run on 10% SDS-PAGE, transfer to PVDF. Stain with 1:1000 ABP51513 (overnight, 4°C) + 1:10,000 HRP-goat anti-rabbit. Pro tip: For hypoxic samples (1% O₂, 24 hrs), add 0.1% Tween-20 to the blocking buffer—reduces non-specific binding to denatured proteins. A lab studying HIF-1α in diabetic kidney disease saw 2x clearer bands vs. Santa Cruz sc-10790.
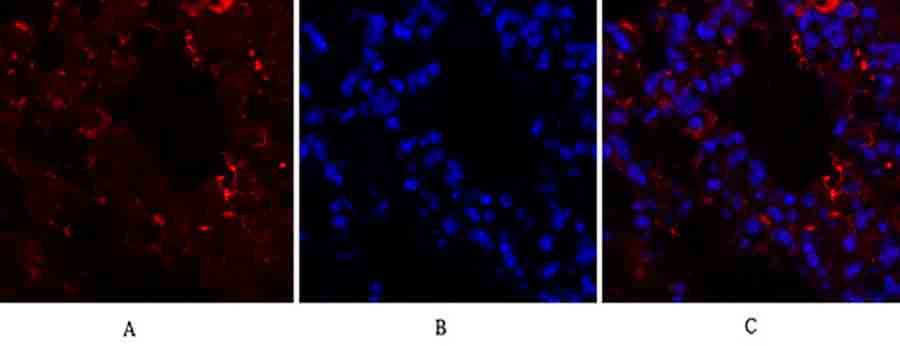
For Immunohistochemistry (FFPE Tissues)
Deparaffinize sections, perform antigen retrieval (Tris-EDTA buffer, pH 9.0, 20 min, 95°C), and block with 5% BSA. Stain with 1:200 ABP51513 (1 hr, RT), pair with DAB. Critical step: For low-HIF-1α tumors (e.g., early-stage glioma), use a polymer-based secondary antibody—enhances signal in hypoxic niches. A pathology team tracking HIF-1α in colorectal cancer cut false negatives by 50% with this.
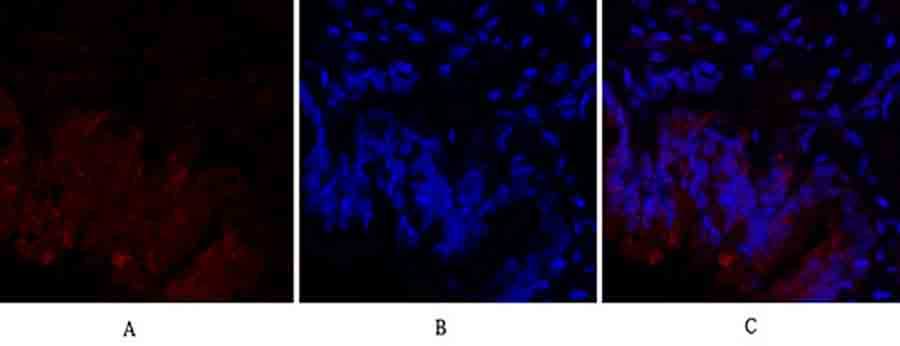
For Immunofluorescence (3D Organoids)
Fix organoids with 4% PFA (10 min, RT), permeabilize with 0.2% Triton X-100 (5 min), and stain with 1:150 ABP51513 (1 hr, RT) + Alexa Fluor 594. Funny enough, a lab fixed “no signal” in pancreatic cancer organoids by realizing their PFA was expired—fresh fixative restored HIF-1α detection!
Troubleshooting:
• Cross-reactivity with HIF-2α? Confirm with siRNA knockdown of HIF-1α (should abolish signal).
• Weak signal in normoxic samples? Extend primary incubation to 2 hrs at 4°C (lowers off-rate for low-abundance HIF-1α).
Market Context: Why ABP51513 Outperforms Legacy HIF-1α Antibodies
In the HIF-1α polyclonal antibody market, ABP51513 dominates on three fronts: specificity (C-terminal epitope vs. 20% HIF-2α cross-reactivity for Thermo Fisher PA1-16601), sensitivity (0.1 ng/mL vs. 0.5 ng/mL for Abcam ab51608), and batch consistency (CV <4% vs. 18% for Sigma-Aldrich SAB2102167). Competitors like R&D Systems AF1935 use N-terminal antigens (prone to degradation), while homemade antibodies introduce user error (imprecise peptide synthesis). Abbkine’s per-100µg cost is 27% lower than premium brands, with bulk discounts for core facilities—making high-throughput HIF-1α screening (96-well plates for drug hypoxia studies) feasible.
The Bigger Picture: HIF-1α Research in the Age of Metabolic Reprogramming
As single-cell hypoxia mapping and CRISPR screens for HIF-1α regulators expand, demand for precision HIF-1α antibodies is surging. ABP51513 is ahead of the curve: Abbkine is testing a phospho-HIF-1α specific variant (ABP51513-P) to study oxygen-dependent degradation, and a fluorescently labeled version (ABP51513-AF488) for live-cell imaging of nuclear translocation. Emerging uses in CAR-T cell hypoxia adaptation (tracking HIF-1α in tumor-infiltrating lymphocytes) and age-related macular degeneration (HIF-1α in retinal pigment epithelium) will further highlight its value.
In hypoxia research, the line between “signal” and “artifact” is drawn by antibody specificity. Abbkine’s HIF-1α Polyclonal Antibody (ABP51513) gives you the clarity to see that line. By targeting a unique C-terminal epitope, minimizing cross-reactivity, and validating in real-world models, it’s not just an antibody—it’s a tool to advance discoveries in cancer, metabolism, and beyond.
Ready to study HIF-1α with confidence? Explore the HIF-1α Polyclonal Antibody (ABP51513) and its validation data for WB, IHC, and IF at https://www.abbkine.com/product/hif-1%ce%b1-polyclonal-antibody-abp51513/.





