




Beyond the Eosinophil Hype: Why Measuring SIGLEC8 Protein Levels Is the Missing Link in Type 2 Inflammation and Next-Gen Asthma Therapeutics
If you still think of Siglec-8 (Sialic acid-binding Ig-like lectin 8) as “just another eosinophil surface marker,” you’re missing the moment it becomes a precision-medicine target. SIGLEC8 is a sialic acid–recognizing inhibitory receptor expressed almost exclusively on eosinophils, basophils, mast cells, and group 2 innate lymphoid cells (ILC2s) — the very cellular axis driving severe asthma, chronic rhinosinusitis with nasal polyps (CRSwNP), eosinophilic granulomatosis with polyangiitis (EGPA), and a spectrum of hypereosinophilic syndromes. What makes it so exciting is that crosslinking Siglec-8 doesn’t just inhibit—it actively programs eosinophil apoptosis and functional shutdown, which is exactly why anti-Siglec-8 therapeutics (e.g., lirentelimab/KB001-A) have moved from “interesting concept” to clinical results. But to translate that biology into rigorous, publishable data, you need more than a flow-plot gated on airway cells—you need a quantitative handle on SIGLEC8 protein itself, whether it’s surface density, a soluble/cleaved ectodomain, or a BAL-fluid biomarker. The Human Sialic acid-binding Ig-like lectin 8 (SIGLEC8) ELISA Kit (KTE60659) from Abbkine is built for exactly that job: a two-site sandwich ELISA that converts this tightly restricted glyco-immune receptor into an interpolated concentration (ng/mL) you can normalize, replicate, and defend across cohorts and conditions.
SIGLEC8 Biology in a Nutshell: Sialoglycans, ITIMs, and Eosinophil Fate
SIGLEC8 (UniProt: O95939, ~62–70 kDa transmembrane glycoprotein) belongs to the CD33-related Siglec family. Its N-terminal V-set domain binds α2,3- and α2,6-linked sialic acid (often presented on glycoproteins/glycolipids), while its cytoplasmic tail harbors two immunoreceptor tyrosine-based inhibitory motifs (ITIMs) that recruit phosphatases (SHP-1/SHP-2) to dampen activating signals.
But here’s the twist researchers exploit: when Siglec-8 is artificially crosslinked (e.g., by multivalent sialoglycan ligands or agonistic antibodies), signaling diverges into a pro-apoptotic/desensitization program in eosinophils—calcium flux, mitochondrial disruption, caspase activation, and cell death. That property is why anti-Siglec-8 mAbs are designed not merely as “blocking” agents but as targeted depletion/modulation tools for eosinophil-driven disease.
Expression-wise, SIGLEC8 is considered highly restricted: strongest on mature blood/tissue eosinophils, detectable on basophils and lung mast cells, and increasingly appreciated on ILC2s in Type 2–inflamed airway mucosa. It is largely absent on neutrophils, T/B cells, and most non-hematopoietic cells—making it a clean, tissue-relevant marker when you need to separate eosinophil-centric biology from background noise.
Why a Sandwich ELISA for SIGLEC8? Because “% Positive by Flow” Isn’t Always Enough
Flow cytometry is king for cellular surface density (MFI) and population gating. Immunofluorescence is gorgeous for spatial proof. But when the scientific claim becomes:
“Airway SIGLEC8 protein is elevated 2.3× in severe asthma vs. controls and drops after anti-Siglec-8 treatment…”
you need a plate-based, absolute-unit readout that doesn’t depend on cell recovery or subjective gating. A sandwich ELISA delivers:
• Two independent epitopes (pre-coated capture vs. biotinylated detection) → far better specificity for a sialoglycoprotein where glycosylation can confound single-antibody approaches.
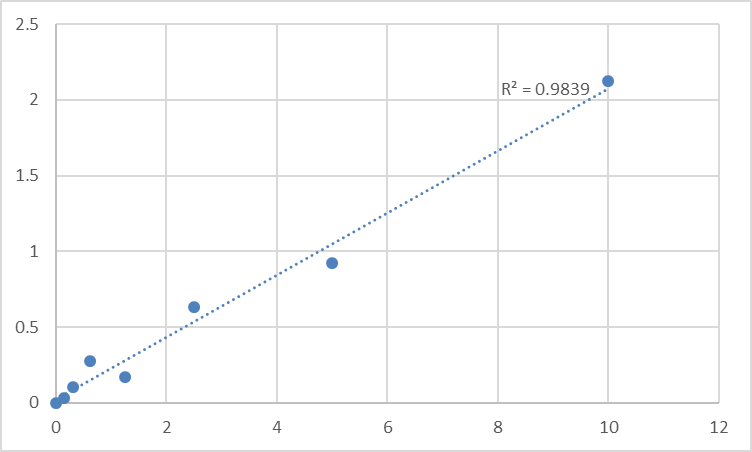
• A recombinant standard curve on every plate → OD₄₅₀ → ng/mL, so your stats actually mean something.
• Scalable throughput for BAL-fluid panels, serum/plasma feasibility studies, or tissue-lysate cohorts where you can’t afford one gel per sample.
This is especially important if you’re chasing the soluble/cleaved SIGLEC8 ectodomain (reported in inflammation contexts) or trying to normalize lysate data to total protein (BCA) to compare across uneven recoveries.
Assay Principle: The KTE60659 Sandwich ELISA, Step by Step
The kit uses the classic, high-specificity two-site sandwich format:
- A 96-well microplate is pre-coated with a capture antibody specific for human SIGLEC8.
- Standards and samples (serum, plasma, BAL fluid, tissue homogenates, cell culture supernatants/lysates, other biological fluids) are added; SIGLEC8 present binds.
- After washing, a biotin-conjugated anti-SIGLEC8 detection antibody (different epitope) forms the sandwich complex.
- Streptavidin–HRP binds biotin → TMB produces blue color ∝ bound SIGLEC8.
- Stop solution turns wells yellow → read Absorbance at 450 nm → interpolate unknowns from the SIGLEC8 standard curve.
Typical assay runtime: ~3–5 hours (varies with incubation timing), and the kit is for Research Use Only (not for diagnostic use in humans).
Performance Snapshot You’ll Commonly See Cited for This Class
Parameter Typical Specification (KTE60659 family)
Target Human SIGLEC8 / Sialoadhesin-like lectin 8 (UniProt O95939)
Format 96-well sandwich ELISA, pre-coated capture
Detection Biotin-Ab → Streptavidin–HRP → TMB, 450 nm read
Dynamic Range 0.156 – 10 ng/mL
Sensitivity / LOD ~0.094 ng/mL
Intra-Assay CV < 8% (often ≤ ~5%)
Inter-Assay CV < 10%
Spike Recovery ~90–105% (matrix-dependent; run your own controls)
Samples Serum, plasma, BAL fluid, tissue homogenates, cell lysates, supernatants
Duration ~3–5 hours
(Confirm exact range/CV/recovery for your lot in the Abbkine manual/certificate of analysis.)
Where Quantifying SIGLEC8 Actually Moves the Needle
- Severe asthma & Type 2 airway diseases (BAL / sputum / tissue)
Quantify SIGLEC8 in BAL fluid or nasal polyp/tissue lysates to tie airway eosinophil activation to clinical severity, fractional exhaled NO (FeNO), or blood eosinophil thresholds. It’s also a natural companion to ECP, EDN, CLC/Gal-10 (Charcot-Leyden crystal protein) or periostin (though periostin is fibroblast-derived, not eosinophil-derived).
- Anti-Siglec-8 therapeutic programs (lirentelimab analogs)
If you’re running preclinical PK/PD or human explant models, you want to measure not just “eosinophils dropped” but whether SIGLEC8 protein in fluid/tissue lysate shifts with treatment—especially if the drug itself might shed or modulate the ectodomain.
- Hypereosinophilic syndromes & EGPA-like models
In rare-disease contexts where patient sample volume is limiting, a sensitive sandwich ELISA can extract a usable ng/mL read from small-volume plasmas/BALs where flow recovery is impractical.
- ILC2–eosinophil crosstalk & in vitro maturation
Track SIGLEC8 in eosinophil purification/maturation cultures or ILC2–eosinophil co-cultures to correlate surface/secreted levels with IL-5, IL-33, TSLP, or viral mimicry (poly I:C/RSV) conditioning.
- Glycobiology controls
Because SIGLEC8 binding depends on sialic acid presentation, ELISA results can be complemented by controlled neuraminidase treatments (external sialidase as experimental variable, not routine handling!) to test whether signal is sialoglycan-sensitive—helpful for a methods-focused paper.
Quick Lab Habits That Keep Your SIGLEC8 Numbers Honest
• Fresh or snap-frozen samples only for soluble/cleaved forms; avoid repeated freeze–thaw (aliquot early).
• Protease inhibitors in BAL/homogenate buffers (PMSF + cocktail), because ectodomains are protease-magnet.
• Normalize lysates to total protein (BCA) and report ng SIGLEC8 / mg total protein when you’re not in a “pure fluid” readout.
• Run the full standard curve on every plate — sialoglycoprotein signals can drift with subtle background differences; the curve is your insurance.
• If you’re comparing blood vs. BAL, remember: circulating SIGLEC8 may reflect differential shedding vs. cellular content; interpret conservatively and pair with a cell-count metric when possible.
The Bottom Line
SIGLEC8 is one of those rare markers that is both a disease-relevant gatekeeper (eosinophil/apoptotic fate) and a tractable therapeutic entry point (agonistic crosslinking / anti-Siglec-8 mAbs). But publishing that story convincingly means measuring it like a scientist, not just gating it. The Human Sialic acid-binding Ig-like lectin 8 (SIGLEC8) ELISA Kit — KTE60659 from Abbkine gives you a pre-coated sandwich ELISA platform that’s sensitive enough for BAL-fluid and lysates, specific enough to survive reviewer scrutiny, and fast enough (~3–5 h) to keep your workflow moving: capture mAb → biotin detection → HRP–TMB → 450 nm → ng/mL.
Product Reference: KTE60659 – Human Sialic acid-binding Ig-like lectin 8 (SIGLEC8) ELISA Kit
Learn more and order: https://www.abbkine.com/product/human-sialic-acid-binding-ig-like-lectin-8-siglec8-elisa-kit-kte60659/
(For Research Use Only; not for diagnostic procedures in humans.)





