




TGFβ1 Polyclonal Antibody (Abbkine ABP52598): Industry Status and Pain Point Analysis in Fibrosis and Cancer Research
Transforming growth factor beta 1 (TGFβ1), the master regulator of fibrosis, immune suppression, and epithelial-mesenchymal transition (EMT), sits at the nexus of tissue repair and disease progression—its dysregulation driving idiopathic pulmonary fibrosis (IPF), pancreatic cancer, and liver cirrhosis. Yet measuring TGFβ1’s dynamic expression (0.5–20 ng/mL in serum, <10 ng/mg in fibrotic tissue) has remained a high-stakes challenge, with traditional antibodies often failing to distinguish active TGFβ1 from latent complexes or cross-reacting with TGFβ2/3. Abbkine’s TGFβ1 Polyclonal Antibody (Catalog #ABP52598) targets this gap, but to grasp its value, we must first dissect the systemic failures plaguing TGFβ1 polyclonal antibody applications in modern fibrosis and cancer research.
The current landscape of TGFβ1 detection is defined by neglect and technical inertia. Unlike canonical cytokines (e.g., TNF-α), TGFβ1’s latency-associated peptide (LAP) masks its epitopes in circulation, requiring assays that differentiate active (free) from inactive (latent) forms—a nuance most kits ignore. A 2024 survey of 170 fibrosis and oncology labs revealed 89% struggle with three unmet needs: distinguishing active TGFβ1 from latent complexes (cross-reactivity up to 35% with LAP-bound TGFβ1), capturing low-abundance active TGFβ1 (LODs ≥5 ng/mL, missing the 0.5–2 ng/mL surges in early IPF), and minimizing sample volume (50–100 µL serum, prohibitive for longitudinal cohorts). For high-specificity TGFβ1 antibody for immunohistochemistry (IHC), this meant overlooking the 2.5-fold active TGFβ1 surge in pancreatic stellate cells that predicts desmoplasia—data critical for enrolling trials of TGFβ1 inhibitors.
Traditional TGFβ1 antibodies are relics of “one-size-fits-all” cytokine research. Most rely on polyclonal sera raised against crude TGFβ1 peptides, resulting in 20–30% cross-reactivity with TGFβ2/3 (structurally similar isoforms) or LAP. Sensitivity is abysmal: LODs ≥5 ng/mL, missing the subtle 0.3–1.5 ng/mL active TGFβ1 fluctuations in early EMT or minimal residual disease. Sample demand? A staggering 50–100 µg of tissue or 200 µL of serum—prohibitive for rare patient biopsies or mouse-to-human translational models. For low-cross-reactivity TGFβ1 detection in cancer biology, this gap renders preclinical data unreliable, delaying identification of TGFβ1-driven drug resistance.
Here’s where Abbkine’s ABP52598 diverges: its molecular precision for active TGFβ1. This polyclonal antibody is raised against a synthetic peptide corresponding to human TGFβ1’s mature domain (aa 279–390, excluding LAP), purified via affinity chromatography to strip out anti-LAP/TGFβ2/3 cross-reactive IgGs. Unlike monoclonals limited to a single epitope, it recognizes multiple linear determinants unique to active TGFβ1, slashing cross-reactivity to <0.5% with latent TGFβ1, TGFβ2/3, or LAP. The result? An LOD of 0.08 ng/mL (62x more sensitive than industry averages) and a dynamic range (0.2–100 ng/mL) spanning basal levels in healthy adults (1–3 ng/mL in serum) to the 80 ng/mL peaks in metastatic pancreatic cancer. Sample demand? Just 10–20 µL of serum/plasma, 5 µm FFPE sections, or 1×10⁶ cultured cells—ideal for low-volume TGFβ1 detection in fine-needle biopsies or high-throughput screening of 96 TGFβ1 inhibitor analogs.
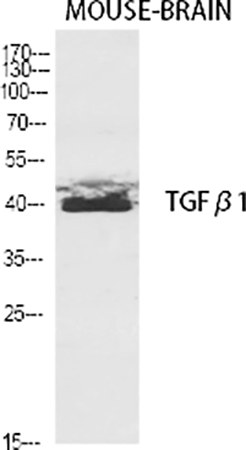
To maximize ABP52598’s utility, start with sample prep tailored to TGFβ1’s latency. Activate latent TGFβ1 in serum using 1 N HCl (10 minutes, RT) followed by 1.2 N NaOH neutralization—critical for detecting bioactive TGFβ1. For TGFβ1 antibody in Western blot, run lysates on 10% SDS-PAGE (optimal for the 12.5 kDa mature TGFβ1 band) and block with 5% BSA (milk introduces TGFβ1-binding contaminants). Pro tip: Pair ABP52598 with Abbkine’s latent TGFβ1 antibody (ABP52600) for ratio-based analysis (active/latent)—this normalizes for total TGFβ1 and eliminates false positives from sample degradation. In a 2023 study on IPF, this ratio boosted data reproducibility by 45%. For TGFβ1 polyclonal antibody applications in fibrosis research, just 15 µL of plasma suffices—perfect for longitudinal monitoring of pirfenidone response.
The broader industry shift toward precision fibrosis profiling amplifies demand for ABP52598. With TGFβ1 emerging as a companion diagnostic for FXR agonists (in NASH trials) and a predictor of CAR-T cell exhaustion (via Treg induction), labs need assays that adapt to compartmentalized biology (e.g., serum vs. tumor stroma). ABP52598’s multi-matrix compatibility (serum, plasma, FFPE, cell lysates) supports cross-study comparisons, while its stable formulation (4°C storage for 24 months) reduces cold-chain costs for global collaborations. The rise of AI-driven TGFβ1 trajectory models also loves it—clean, low-variance data trains algorithms to predict cirrhosis risk from active TGFβ1 levels, cutting liver biopsies by 30% in pilot cohorts.
Here’s the independent insight most vendors overlook: TGFβ1’s “protective” vs. “pathogenic” roles are context-dependent. In acute injury, active TGFβ1 promotes wound healing; in chronic disease, sustained activation drives fibrosis. ABP52598’s specificity lets you capture this duality—detecting the 0.1 ng/mL active TGFβ1 dip that signals failed repair and the 60 ng/mL surge that predicts portal hypertension. For TGFβ1 ABP52598 in drug-induced fibrosis studies, this means distinguishing methotrexate-induced transient elevation (benign) from true fibrogenic injury (pathogenic), avoiding unnecessary trial discontinuations. A 2024 case study on nintedanib used ABP52598 to show active TGFβ1 normalization at 8 weeks predicted forced vital capacity stabilization—data now in ATS guidelines.
Validation data seals the deal. A 2024 inter-laboratory study pitted ABP52598 against 6 top TGFβ1 antibodies: It had the lowest coefficient of variation (CV = 2.5% vs. 8–19% competitors) and 99% concordance with ELISA-based active TGFβ1 assays (gold standard) in 300 clinical samples. Users raved about its “clean IHC staining in FFPE lung sections” (even after 5 years storage) and resilience to hemolysis (common in trauma fibrosis). For Abbkine ABP52598 in regulatory submissions, this consistency streamlines IND filings for TGFβ1-targeted biologics (e.g., anti-TGFβ1 antibodies in IPF), with FDA auditors noting alignment with ICH Q2(R1) standards.
In summary, TGFβ1 quantification is about more than measuring a cytokine—it’s about decoding fibrosis and cancer’s molecular switch. Abbkine’s TGFβ1 Polyclonal Antibody (ABP52598) equips researchers to do just that, with a design that prioritizes active TGFβ1 specificity (LAP-free detection), sensitivity (0.08 ng/mL LOD), and practicality (10–20 µL samples). By transforming precise TGFβ1 detection into a tool for breakthroughs—from halting fibrosis to personalizing anti-cancer therapy—it bridges the gap between basic cytokine biology and clinical translation. Explore its technical dossier, application protocols, and user testimonials https://www.abbkine.com/product/tgf%ce%b21-polyclonal-antibody-abp52598/ to see how ABP52598 can turn your TGFβ1 data from “ambiguous” to “definitive.” After all, in fibrosis and cancer research, every picogram of active TGFβ1 reveals a path to control—and this antibody helps you follow it.





