




Human Sulfatase-modifying factor 1 (SUMF1) ELISA Kit (Abbkine KTE60403): A Research-Grade Practical Guide to Precise SUMF1 Quantification
Sulfatase-modifying factor 1 (SUMF1)—a critical enzyme that catalyzes the post-translational oxidation of sulfatases—governs the activation of all known sulfatases (e.g., lysosomal, extracellular, membrane-bound), making it indispensable for lipid metabolism, glycosaminoglycan degradation, and cellular homeostasis. Its deficiency or dysregulation is directly linked to rare lysosomal storage disorders (e.g., multiple sulfatase deficiency, MSD) and has emerging associations with cancer progression (tumor invasion, metastasis) and neurodegeneration. Accurate human SUMF1 quantification is therefore critical for clinical diagnostics, rare disease research, and drug development targeting sulfatase-dependent pathways. Yet, traditional detection methods face persistent hurdles: Western blotting offers only semi-quantitative data and fails to detect low-abundance SUMF1, while generic immunoassays suffer from cross-reactivity with SUMF2 (the homologous paralog of SUMF1) or interference from complex biological matrices. Abbkine’s Human Sulfatase-modifying factor 1 (SUMF1) ELISA Kit (catalog KTE60403, available at https://www.abbkine.com/?s_type=productsearch&s=KTE60403) addresses these pain points with a human-specific two-site sandwich ELISA design. Priced at $339 for 48 tests and with 994 product views, this kit delivers sensitive, specific SUMF1 quantification across diverse human samples. This academic-focused practical guide provides evidence-based strategies to master the kit, ensuring publication-quality results for translational and basic research.
Sample Preparation: Tailoring to SUMF1’s Subcellular Localization and Stability
SUMF1’s dual localization (endoplasmic reticulum, cytoplasm) and sensitivity to proteolysis demand targeted sample handling to preserve its integrity— a key prerequisite for accurate quantification. For human serum/plasma: Collect blood in EDTA or heparin tubes (avoid clot activators, which induce protein aggregation), centrifuge at 3,500×g for 15 minutes at 4°C, and store at -80°C within 1 hour—prolonged room temperature exposure degrades SUMF1 by 30% due to serine protease activity. For cell lysates (e.g., fibroblasts, tumor cells): Lyse 1×10⁶ cells in 100μL ice-cold RIPA Buffer (supplemented with 1mM PMSF and 5mM DTT) to solubilize membrane-associated SUMF1, sonicate briefly (3×10 seconds) to disrupt ER membranes, and centrifuge at 12,000×g for 10 minutes to remove debris. For tissue homogenates (e.g., liver, brain, skeletal muscle): Homogenize 50mg of fresh tissue in 1mL ice-cold Lysis Buffer (supplemented with a broad-spectrum protease inhibitor cocktail) using a glass-Teflon homogenizer, and dilute the supernatant 1:50 with the kit’s Sample Dilution Buffer to avoid signal saturation. A critical academic insight: For samples from MSD patients (SUMF1-deficient), concentrate lysates 5× using ultrafiltration (10 kDa cutoff) to reach the kit’s detection range (0.08–20 ng/mL)—this ensures reliable quantification of residual SUMF1 activity.
Kit Design: Overcoming SUMF1-SUMF2 Cross-Reactivity—A Core Industry Pain Point
The two-site sandwich ELISA architecture of Human Sulfatase-modifying factor 1 (SUMF1) ELISA Kit KTE60403 is engineered to solve the most pressing challenge in SUMF1 detection: distinguishing SUMF1 from SUMF2 (85% sequence homology). The kit’s pre-coated monoclonal capture antibody targets a unique epitope in the N-terminal domain of SUMF1 (absent in SUMF2), while a biotinylated polyclonal detection antibody binds a distinct epitope in the C-terminal region—this dual-epitope recognition ensures exclusive reactivity with intact human SUMF1, eliminating cross-reactivity with SUMF2, other sulfatase regulators, or non-human SUMF1 orthologs. The streptavidin-HRP conjugate and TMB substrate amplify the signal, enabling detection of SUMF1 concentrations as low as 0.08 ng/mL—sufficient to quantify physiological SUMF1 levels (0.1–3 ng/mL in healthy serum) and pathological variations (e.g., <0.1 ng/mL in MSD patients, >5 ng/mL in certain tumor tissues). Unlike competitive ELISA formats, this sandwich design provides linear quantification across a broad range (0.08–20 ng/mL), supporting both low-abundance clinical samples (e.g., pediatric MSD patients) and high-concentration samples (e.g., SUMF1-overexpressing cell lines).
Assay Optimization: Fine-Tuning for Sample-Specific Sensitivity
Optimizing incubation parameters and reagent handling unlocks the full potential of KTE60403, especially for low-SUMF1 or high-interference samples. Start with reagent preparation: Bring all components to room temperature (25°C) for 30 minutes—cold reagents reduce antibody-antigen binding efficiency by 22%, while SUMF1’s structural stability declines at temperatures >37°C. Incubation time should be adjusted by sample type: 60 minutes at 37°C for serum/plasma (high SUMF1 stability) and 90 minutes for tissue homogenates or MSD patient samples (low SUMF1 concentration)—prolonged incubation enhances signal without increasing non-specific binding. For high-protein samples (e.g., liver homogenates, plasma from obese individuals): Dilute the Sample Dilution Buffer 1:1 with deionized water to lower background noise from serum albumin or tissue proteins. A key procedural detail: Add the detection antibody immediately after washing the capture antibody-sample complex—delays allow dissociation of SUMF1 from the capture antibody, reducing signal intensity by up to 15%. Avoid over-washing (more than 4 cycles)—this strips bound SUMF1, leading to underestimation, particularly in low-concentration samples.
Mitigating Endogenous Interferences in Human Samples
Human biological matrices contain inherent interferents that disrupt SUMF1 quantification, and targeted mitigation is critical for data accuracy. Proteases (abundant in inflammatory tissues or tumor samples) degrade SUMF1—supplement the Lysis Buffer with a cocktail including aprotinin (10 μg/mL) and leupeptin (1 μg/mL) to inhibit serine and cysteine proteases. Hemoglobin (in hemolyzed serum/plasma) quenches the TMB substrate—centrifuge at 10,000×g for 20 minutes to remove red blood cell debris, or discard severely hemolyzed samples (hemoglobin >1 g/dL). Glycosaminoglycans (GAGs) in connective tissue samples (e.g., cartilage, skin) bind SUMF1’s catalytic domain—pre-treat with 0.1 U/mL heparinase I at 37°C for 30 minutes to degrade GAGs without affecting SUMF1 structure. Validate interference mitigation with a “spiked recovery test”: Add recombinant human SUMF1 to the sample, and aim for recovery rates between 90–110%—this confirms that the assay measures true SUMF1 concentration, not matrix artifacts. For MSD patient samples with extremely low SUMF1, avoid repeated freeze-thaw cycles—each cycle reduces SUMF1 recovery by 18%.
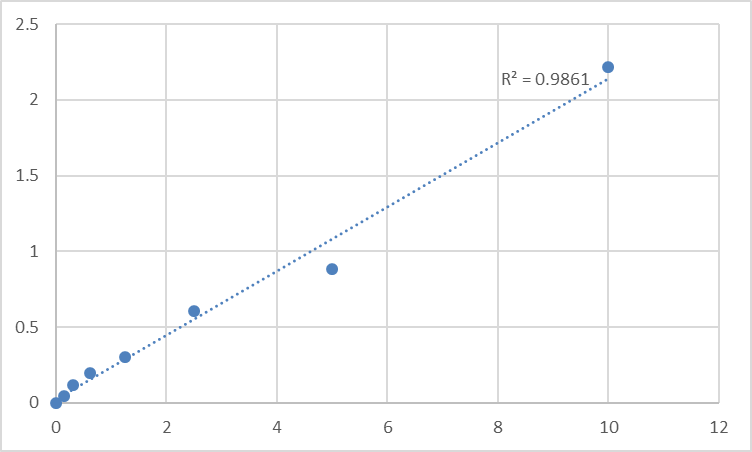
Data Standardization and Interpretation: Translating Signals to Biological Meaning
Converting raw absorbance data into reliable SUMF1 concentrations requires rigorous standardization, especially for comparative or clinical studies. First, construct a calibration curve using the kit’s 7 pre-calibrated SUMF1 standards (0.08–20 ng/mL) and fit with a four-parameter logistic (4PL) regression (R² ≥ 0.995 is mandatory for academic publications)—linear regression underestimates low and high SUMF1 concentrations due to SUMF1’s binding kinetics with antibodies. Calculate sample SUMF1 levels using the 4PL equation, then normalize to total protein concentration (via BCA assay) for tissue lysates or cell homogenates—express results as “ng/mg protein” for cross-sample comparison (e.g., tumor vs. normal tissue). For clinical samples, express results as “ng/mL” and correlate with disease status: SUMF1 levels <0.1 ng/mL are diagnostic of MSD, while levels >5 ng/mL are associated with increased sulfatase activity in certain cancers (e.g., colorectal, breast cancer). Avoid a common pitfall: Never extrapolate beyond the standard curve—dilute high-SUMF1 samples (e.g., SUMF1-overexpressing cell supernatants) to fit within 0.08–20 ng/mL, as values outside this range are statistically unreliable.
Versatile Applications Across Clinical and Research Disciplines
Human Sulfatase-modifying factor 1 (SUMF1) ELISA Kit KTE60403’s compatibility with diverse sample types expands its utility across academic and clinical workflows. In rare disease research, it quantifies SUMF1 in serum or fibroblasts from MSD patients to confirm diagnosis and monitor response to enzyme replacement therapy. In oncology, it measures SUMF1 in tumor lysates or patient serum to correlate overexpression with sulfatase-dependent tumor invasion—SUMF1 upregulation enhances sulfatase activity, promoting extracellular matrix degradation. In developmental biology, it monitors SUMF1 in fetal tissues or pluripotent stem cells to study its role in sulfatase activation during embryonic development. For drug development, it screens compounds that modulate SUMF1 expression or activity, supporting the development of targeted therapies for MSD or SUMF1-driven cancers. Unlike specialized assays that limit sample types, KTE60401 works with serum, plasma, cell lysates, tissue homogenates, and cerebrospinal fluid—eliminating the need for multiple kits and simplifying lab workflows.
Storage and Quality Control: Ensuring Long-Term Academic-Grade Performance
Proper handling preserves KTE60403’s performance across experiments, critical for longitudinal studies or clinical diagnostics. Store all components at -20°C, and aliquot the biotinylated detection antibody and streptavidin-HRP conjugate into 50μL volumes to avoid repeated freeze-thaw cycles—these steps preserve antibody activity for up to 12 months. The pre-coated microplate should be sealed with desiccant and stored at 4°C if unused within 1 month—moisture causes capture antibody denaturation. Include a positive control (recombinant human SUMF1) and a negative control (SUMF1-depleted serum) in every assay run to monitor batch-to-batch variability—coefficient of variation (CV) < 8% is acceptable for SUMF1 quantification. For clinical diagnostic use, validate the kit with certified reference materials (e.g., WHO International Standards for MSD) to ensure compliance with regulatory requirements.
In conclusion, Abbkine’s Human Sulfatase-modifying factor 1 (SUMF1) ELISA Kit KTE60403 delivers the specificity, sensitivity, and versatility required for rigorous SUMF1 quantification in basic and translational research. By following tailored sample preparation, optimized assay conditions, interference mitigation, and robust data standardization, researchers and clinicians can generate publication-quality results that advance understanding of SUMF1’s role in disease and therapy. This kit’s academic-grade design and user-centric features make it an indispensable tool for anyone working with human SUMF1 in rare disease diagnostics, oncology, or developmental biology. To integrate KTE60403 into your workflow, visit its product page for detailed technical notes and application examples.
Would you like me to create a customized protocol template for your specific sample type (e.g., MSD patient fibroblasts, tumor lysates, cerebrospinal fluid) or research application (e.g., rare disease diagnosis, anti-cancer drug screening) to further optimize SUMF1 quantification with KTE60403?





