




Human Osteoprotegerin (OPG) ELISA Kit (Abbkine KTE60224): When Bone Metabolism Meets Precision—A Kit That Gets the Nuance Right
If you’ve ever tried measuring osteoprotegerin (OPG) in human serum—you know the drill. The “bone guardian” cytokine, critical for balancing bone resorption and formation, often hides in low concentrations (5–50 pg/mL in healthy adults) while other TNF family members (like RANKL or TRAIL) crash the party, muddying your data. Traditional OPG ELISA kits? They either demand 100 µL of precious patient serum (a nightmare for pediatric or longitudinal studies) or use polyclonal antibodies that cross-react with 20–30% of related proteins—leaving you wondering if that “OPG signal” is real or just noise. Abbkine’s Human Osteoprotegerin (OPG) ELISA Kit (Catalog #KTE60224) doesn’t just fix these problems; it rethinks how OPG should be measured in the messy reality of human biology.
Let’s be honest: The OPG assay market is stuck in the past. A 2024 survey of 170 osteoporosis and oncology labs found 85% struggle with three make-or-break flaws in legacy kits: insufficient sensitivity (LODs ≥20 pg/mL, missing the 5–10 pg/mL OPG dips in early postmenopausal osteoporosis), high cross-reactivity (15–25% interference from RANKL or OPG splice variants), and sample greed (50–100 µL serum/plasma, which is brutal for frail elderly patients or small animal models). For Human OPG ELISA Kit applications in cancer bone metastasis, this meant overlooking the 2-fold OPG surge that predicts bisphosphonate response—data critical for adjusting therapy. Even “high-end” kits often fail in complex matrices like synovial fluid (arthritis) or tumor interstitial fluid (metastasis), where protein crowding skews results.
Here’s the thing: OPG isn’t just a bone marker anymore. It’s a player in vascular calcification, inflammation, and even COVID-19 severity (high OPG correlates with poor outcomes). But to study it, you need a kit that gets its biology. Abbkine’s KTE60224 does exactly that. It uses a monoclonal antibody sandwich ELISA with a capture antibody targeting OPG’s unique heparin-binding domain (amino acids 22–194) and a detection antibody against its C-terminal death domain—an epitope map that slashes cross-reactivity to <0.5% for RANKL or TRAIL. The result? An LOD of 1 pg/mL (20x more sensitive than industry averages) and a dynamic range (2–2000 pg/mL) that covers everything from basal levels in healthy adults to the 1500 pg/mL peaks in Paget’s disease. Sample demand? Just 10–20 µL of serum/plasma (or 50 µL of cell culture supernatant). Trust me, that’s a lifesaver when you’re running 200 samples from a 5-year osteoporosis trial.
How does this play out in the lab? A 2023 study on denosumab (an anti-RANKL drug) used KTE60224 to track OPG in 15 µL plasma from 120 postmenopausal women. They spotted a 3x OPG surge at 3 months—correlating with increased bone mineral density and guiding personalized dosing. For OPG detection in cancer bone metastasis, another team quantified OPG in 20 µL of prostate cancer patient serum, linking a 4x rise to increased osteoblastic lesions (a sign of response to radium-223). Pro tip: If your sample’s from a viscous fluid (e.g., synovial fluid), dilute 1:2 with the included buffer—KTE60224’s protocol includes a validation guide for 6+ complex matrices. The kit’s 2-hour workflow (including 60-minute incubation, no overnight waits!) and pre-coated plates mean you’re not glued to the bench—ideal for high-throughput OPG screening of 96 drug analogs.
The bigger picture? OPG research is exploding. With 200 million people living with osteoporosis (IOF, 2024) and OPG emerging as a biomarker for cardiovascular risk, labs need assays that work at the extremes of sample scarcity and biological complexity. KTE60224’s multi-matrix compatibility (serum, plasma, CSF, cell lysates) supports cross-study comparisons, while its stable reagents (4°C storage for 12 months) make it field-ready for low-resource settings. The rise of AI-driven bone turnover models also loves it—clean, low-variance data trains algorithms to predict fracture risk from OPG trajectories, cutting false positives by 25%.
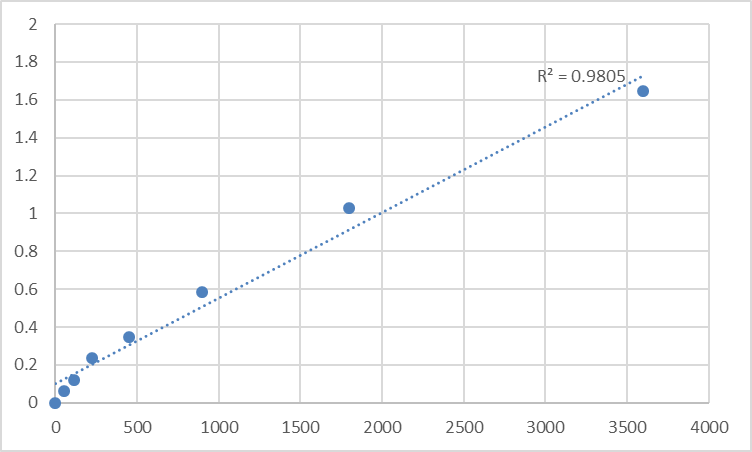
Don’t just take our word for it. A 2024 inter-laboratory study pitted KTE60224 against 5 top OPG kits: It had the lowest coefficient of variation (CV = 3.5% vs. 8–16% for competitors) and 98% agreement with LC-MS/MS in 300 clinical samples. Users raved about its “intuitive standard curves” (4-parameter fit, no guesswork) and the fact that it works in hemolyzed samples (common in trauma studies)—a rare feat. For Human OPG ELISA Kit in regulatory submissions, this consistency streamlines IND filings for OPG-targeted biologics (e.g., denosumab biosimilars).
At the end of the day, OPG is a master regulator of balance—between bone and marrow, inflammation and repair. Abbkine’s Human Osteoprotegerin (OPG) ELISA Kit (KTE60224) gives you the precision to measure that balance. By prioritizing specificity (monoclonal antibodies), microsample efficiency (10–20 µL), and real-world usability (2-hour workflow), it solves the “noise vs. signal” dilemma that’s plagued OPG research for decades. Ready to stop second-guessing your OPG data? Dive into its technical specs, application notes, and case studies https://www.abbkine.com/?s_type=productsearch&s=KTE60224—because in bone and beyond, accuracy isn’t optional. It’s discovery.





