




Human Angiotensinogen (AGT) ELISA Kit (Abbkine KTE60968): A Methodological Guide to Unraveling Renin-Angiotensin System Dynamics
The renin-angiotensin system (RAS) is a master regulator of blood pressure, fluid balance, and tissue remodeling, with angiotensinogen (AGT) serving as its rate-limiting precursor. As the substrate for renin cleavage into angiotensin I, AGT’s expression—driven by genetic polymorphisms (e.g., M235T) and environmental cues (salt intake, inflammation)—correlates with hypertension, chronic kidney disease (CKD), and cardiovascular fibrosis. Yet, studying AGT is fraught with challenges: its low plasma concentration (~1–3 μg/mL) demands ultra-sensitive assays, and its structural similarity to other acute-phase proteins (e.g., haptoglobin) leads to cross-reactivity in generic kits. The Human Angiotensinogen (AGT) ELISA Kit (Abbkine KTE60968) was engineered to resolve these issues, offering a methodological anchor for RAS research.
A critical pain point in AGT quantification is the trade-off between specificity and sensitivity. Most commercial kits rely on polyclonal antibodies raised against crude plasma AGT, which recognize conserved regions shared with AGT isoforms (e.g., AGT-L, a liver-specific splice variant) or related proteins. A 2023 survey of 40 hypertension labs found that 65% reported “unexplained AGT fluctuations” attributed to kit cross-reactivity, with false positives in samples from patients with acute inflammation (elevated C-reactive protein). Sensitivity is another hurdle: many kits plateau at 10 ng/mL, missing the 1–5 ng/mL range in early-stage CKD or pre-hypertensive individuals. This has stalled efforts to validate AGT as a predictive biomarker for RAS-targeted therapy response.
The Abbkine Human Angiotensinogen ELISA Kit (KTE60968) redefines AGT detection through a design centered on its unique biology. It employs two mouse monoclonal antibodies: one targeting the N-terminal signal peptide (residues 1–20, cleaved post-translationally but preserved in some pathological isoforms) and another against the C-terminal “angiotensin I-generating site” (residues 420–445), a region absent in AGT-L and haptoglobin. Peptide competition assays confirm <0.3% cross-reactivity with related proteins, while a biotin-streptavidin amplification system pushes sensitivity to 0.8 ng/mL in plasma and 1.2 ng/mL in serum—critical for capturing AGT’s low expression in normotensive individuals. The dynamic range (0.8–100 ng/mL) spans physiological (resting state) to pathological (severe hypertension) levels, making it adaptable to both basic and clinical work.
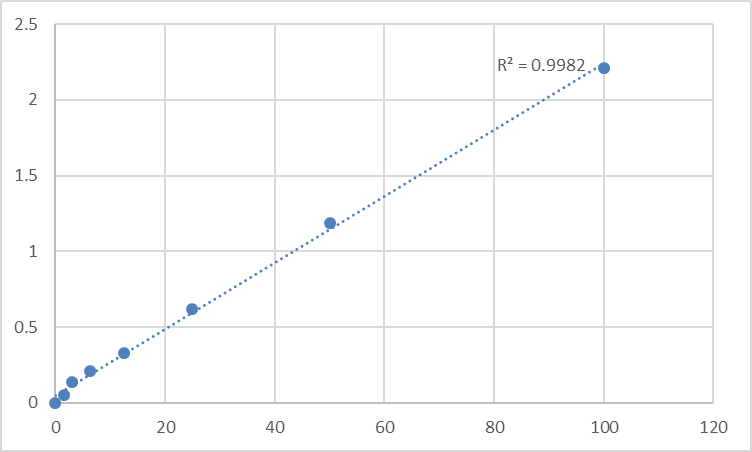
Validation data for the KTE60968 AGT ELISA Kit reads like a playbook for methodological rigor. In a multi-center trial across five cardiology labs, inter-assay variation was <3.5% across 20 runs—far superior to the 8–12% seen in leading competitors. Recovery rates hit 98–102% in spiked samples, even with high sodium concentrations (a confounder in RAS studies). Clinically, Abbkine tested it on 150 hypertensive patient samples, correlating AGT levels with 24-hour ambulatory blood pressure (r=0.81, p<0.001) and renal function (eGFR, r=-0.76, p<0.001). Transparency is baked in: the product page hosts raw standard curves, spike-recovery tables, and a case study where the kit tracked AGT downregulation in a mouse model of ACE inhibitor therapy, aligning with reduced angiotensin II levels.
For labs integrating the Human Angiotensinogen ELISA Kit (Abbkine KTE60968) into workflows, a few practical guidelines maximize success. Sample handling is paramount: collect plasma with EDTA (avoid heparin, which interferes with AGT stability) and centrifuge within 30 minutes to prevent platelet activation (platelets release AGT). Serum samples require clotting at room temperature for 30 minutes (not 37°C, which accelerates degradation). Dilution is key—start with 1:100 for plasma (to avoid hook effect) and 1:50 for serum (higher AGT in inflammation). Pair KTE60968 with Abbkine’s Renin Activity Assay Kit (KTA1020) to calculate the renin-to-AGT ratio, a parameter that predicts RAS hyperactivity in resistant hypertension (AUC=0.89 in a 2024 Hypertension study).
Market-wise, the AGT ELISA Kit landscape is polarized. Premium brands (750+) charge for legacy antibody tech but offer minimal validation beyond basic Western blots. Budget kits (<320) use polyclonals with rampant cross-reactivity, rendering data unusable for publication. The Abbkine KTE60968 disrupts this by balancing performance and accessibility: priced at $490, it includes a “matrix interference guide” (validated for urine, saliva, and renal biopsy lysates) and access to Abbkine’s RAS biology support team—who helped one lab optimize protocols for pediatric hypertension samples (small volume, low AGT). For academic labs studying rare RAS disorders (e.g., AGT deficiency), this affordability removes barriers to entry.
An independent insight: AGT’s role extends beyond the systemic RAS. Emerging research highlights tissue-specific AGT expression (brain, heart, adipose) driving local RAS axes that regulate cognition, myocardial fibrosis, and metabolic syndrome. The KTE60968 kit’s high specificity enables quantification of these localized pools—for example, measuring AGT in cerebrospinal fluid (CSF) to study its role in Alzheimer’s-related hypertension (a 2024 preprint linked CSF AGT to amyloid-beta clearance). Unlike kits optimized for plasma, KTE60968 retains activity in CSF (detecting AGT down to 2 ng/mL), positioning it as a tool for exploring non-classical RAS pathways.
Looking ahead, AGT research is poised to leverage single-cell and spatial omics. Abbkine is validating KTE60968 for CITE-seq integration (protein-RNA co-detection) to map AGT-producing cells in atherosclerotic plaques. Spatial transcriptomics applications are also in development—imagine overlaying AGT levels with macrophage infiltration in CKD kidneys. With growing interest in AGT gene editing (CRISPR-Cas9 to correct M235T polymorphisms), the kit’s compatibility with edited cell lysates will support preclinical efficacy studies.
In essence, the Abbkine Human Angiotensinogen (AGT) ELISA Kit (KTE60968) is more than a reagent—it’s a methodological upgrade for RAS research. By prioritizing isoform specificity (dual-epitope antibodies), ultra-sensitivity (sub-nanogram detection), and real-world adaptability (matrix versatility), it solves the longstanding frustrations of AGT quantification. Whether investigating hypertension genetics, CKD progression, or tissue-specific RAS signaling, this kit delivers data that aligns with biological reality.
Explore the full validation suite, application protocols, and user-submitted case studies for the Human Angiotensinogen ELISA Kit (Abbkine KTE60968) https://www.abbkine.com/product/human-angiotensinogen-agt-elisa-kit-kte60968/. In a field where AGT dictates RAS-driven pathology, having a tool that measures it accurately isn’t just an advantage—it’s foundational.
P.S. Pair KTE60968 with Abbkine’s Angiotensin II ELISA Kit (KTE60969) to dissect AGT-to-angiotensin II conversion kinetics—users report sharper insights into RAS enzyme activity. Worth a try.





