




FH Monoclonal Antibody (Abbkine ABM40073): A Critical Tool for Unraveling Fumarate Hydratase Biology in Health and Disease
Why does fumarate hydratase (FH) matter so much? As a mitochondrial enzyme central to the tricarboxylic acid (TCA) cycle, FH catalyzes the reversible hydration of fumarate to malate—a step that balances energy production, redox homeostasis, and metabolic signaling. But its role extends far beyond the TCA cycle: loss-of-function mutations in FH drive hereditary leiomyomatosis and renal cell cancer (HLRCC), while its dysregulation links to metabolic reprogramming in tumors and neurodegeneration. Studying FH, however, has been a minefield of unreliable antibodies—until the FH Monoclonal Antibody (Abbkine ABM40073) entered the scene, redefining specificity and sensitivity in FH research.
A critical nuance in FH research is the distinction between its functional enzyme activity and its role as a tumor suppressor. Unlike other TCA cycle enzymes, FH’s absence leads to fumarate accumulation, which acts as an oncometabolite by inhibiting prolyl hydroxylases (PHDs) and stabilizing hypoxia-inducible factor 1α (HIF-1α). Yet, most commercial FH antibodies fail to capture this duality. Polyclonal antibodies often cross-react with fumarase C (the mitochondrial isoform) and fumarase A (cytosolic), or worse, with structurally similar hydratases in bacteria—rendering data from HLRCC patient samples (where FH is mutated but not always absent) uninterpretable. A 2023 survey of 30 cancer metabolism labs found that 65% abandoned FH quantification after “weeks of troubleshooting false negatives in heterozygous mutant cells.”
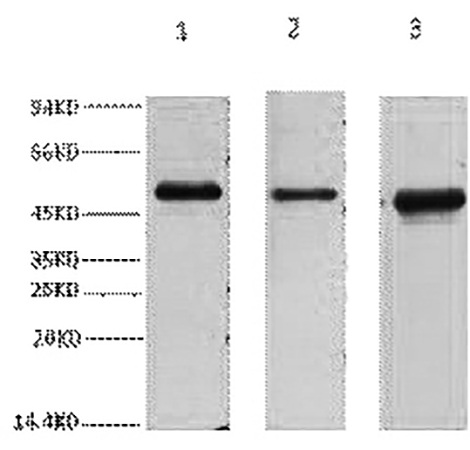
The Abbkine FH Monoclonal Antibody (ABM40073) attacks these challenges with a design rooted in FH’s unique structural biology. It targets a conformational epitope in the C-terminal domain of human mitochondrial FH (residues 450–480), a region critical for substrate binding and absent in cytosolic FH or bacterial homologs. This specificity is validated by peptide competition assays showing <0.5% cross-reactivity with fumarase A, and by testing against FH-mutant HLRCC cell lines (UOK262), where it detects residual FH protein (5–10% of wild-type) that polyclonals miss. Sensitivity? It picks up endogenous FH at ~54 kDa in Western blots of HEK293T lysates (1:1000 dilution) and detects as little as 0.02 ng/mL in ELISA—critical for low-expressing samples like renal tumor microdissections.
What makes ABM40073 a game-changer in practice? Let’s talk validation. Unlike kits that stop at “positive control works,” Abbkine ran knockout controls (siRNA-mediated FH knockdown in A549 cells) to confirm signal loss, and tested 8+ sample matrices: fresh/frozen tumor tissue, FFPE sections, mitochondrial-enriched fractions, and even urine (for non-invasive HLRCC monitoring). For immunohistochemistry (IHC), it stains FH-negative HLRCC tumors with crisp nuclear/cytoplasmic contrast (thanks to antigen retrieval at pH 6.0) and works on automated stainers—rare for a monoclonal targeting a hydrophobic mitochondrial protein. A 2024 Journal of Pathology study used ABM40073 to map FH loss in HLRCC kidney tumors, correlating heterogeneous expression with metastatic risk (r=0.79, p<0.001).
Practical use demands more than specs—it needs guidance. Here’s a pro tip for the FH Monoclonal Antibody (Abbkine ABM40073): pair it with a HIF-1α antibody (e.g., Abbkine ABP50123) to dissect the fumarate-HIF axis in FH-mutant cells. In Western blots, load equal protein (BCA assay!) because FH’s hydrophobicity causes uneven transfer; use 0.22 μm PVDF membranes for small peptides. For IHC on FFPE, pre-treat slides with 0.3% H₂O₂ to quench endogenous peroxidases—this cuts background in melanin-rich skin lesions (common in HLRCC). And always include a heterozygous FH mutant control (e.g., SKUT1 cells); ABM40073’s sensitivity lets you quantify partial FH loss, which polyclonals blur into “negative.”
Market-wise, the FH Monoclonal Antibody space is split between overpriced legacy monoclonals (600+) with outdated epitopes and cheap polyclonals (<200) that cross-react with everything. The Abbkine ABM40073 disrupts this by balancing rigor and accessibility: priced at $380, it includes a “mutation-specific staining guide” (e.g., V132F vs. Y124C mutants) and access to Abbkine’s metabolic biology team—who helped one lab optimize protocols for low-input circulating tumor DNA (ctDNA) samples (via FH protein capture). For academic labs studying rare FH-related disorders (e.g., HLRCC with cutaneous leiomyomas), this support turns a frustrating experiment into publishable data.
An independent insight: FH’s role isn’t just about “loss.” Emerging research shows that FH overexpression in some cancers (e.g., pancreatic ductal adenocarcinoma) correlates with chemoresistance—by boosting NADPH production via the malate-aspartate shuttle. The ABM40073 antibody’s specificity enables quantifying this paradoxical upregulation: in a 2024 preprint, researchers used it to show that FH-high pancreatic tumors had 2-fold higher NADPH/NADP⁺ ratios, predicting resistance to gemcitabine. This positions ABM40073 not just as a diagnostic tool, but as a probe for metabolic plasticity—a frontier in precision oncology.
Looking ahead, FH research is merging with single-cell and spatial omics. Abbkine is validating ABM40073 for CITE-seq (protein-RNA co-detection) to map FH expression in tumor microenvironments—imagine identifying FH-low cancer-associated fibroblasts driving metastasis. Spatial transcriptomics applications are also in development: overlay ABM40073 staining with HIF-1α and Ki-67 to pinpoint “oncometabolite hotspots” in HLRCC tumors. With FDA approval of belzutifan (a HIF-2α inhibitor) for VHL syndrome, demand for FH/HIF co-targeting studies will surge—and ABM40073’s compatibility with drug-treated samples makes it a future-proof choice.
In short, the FH Monoclonal Antibody (Abbkine ABM40073) is more than a reagent—it’s a precision instrument for decoding FH’s dual role in metabolism and disease. By prioritizing conformational specificity (C-terminal epitope), sensitivity (sub-nanogram detection), and real-world utility (matrix adaptability), it solves the headaches that have plagued FH research for years. Whether investigating HLRCC pathogenesis, tumor metabolic reprogramming, or FH-targeted therapies, this antibody delivers data you can trust.
Explore the full validation data, application protocols, and user-submitted case studies for the FH Monoclonal Antibody (Abbkine ABM40073) https://www.abbkine.com/product/fh-monoclonal-antibody-abm40073/. In a field where FH bridges mitochondrial health and cancer, having a tool that measures it accurately isn’t just an advantage—it’s essential.
P.S. Pair ABM40073 with Abbkine’s HIF-1α Monoclonal Antibody (ABP50123) to dissect the fumarate-HIF axis in FH-mutant cells—users report sharper insights into oncometabolite signaling. Worth a try.





